Late Breaking Clinical Trials
Virtual Recording

Robin Nijveldt, MD, PhD
Prof. Dr.
Radboud University Medical Center
Nijmegen, Gelderland, Netherlands
Robin Nijveldt, MD, PhD
Prof. Dr.
Radboud University Medical Center
Nijmegen, Gelderland, Netherlands
Michael Maeng
Dr.
Aarhus University Hospital, Denmark
Casper Beijnink
Dr.
Radboudumc, Netherlands
Jan Piek
Prof. Dr.
Amsterdam Medical Center
Amsterdam, Netherlands
Rasha Al-Lamee, MD, PhD
Dr.
National Heart and Lung Institute, Imperial College London
London, United Kingdom
Luis Raposo
Dr.
Hospital de Santa Cruz, Portugal
Sergio Bravo Baptista
Dr.
Hospital Prof Fernando da Fonseca, Portugal
Javier Escaned
Prof. Dr.
Hospital Clínico San Carlos, Spain
Justin Davies
Prof. Dr.
Monaco Cardio, Monaco
Igor Klem, MD
Dr.
Duke Cardiovascular Magnetic Resonance Center
Durham, North Carolina, United States
Abdelilah el Barzouhi
Dr.
Haaglanden Medical Center, Netherlands
Mustafa Ilhan
Dr.
Zuyderland Medical Center, Netherlands
Stijn Brinckman
Dr.
Tergooi Hospitals, Netherlands
Dan Jones
Dr.
Barts Health NHS Trust, United Kingdom
.jpg "Tomaž Podlesnikar, MD photo")
Tomaž Podlesnikar, MD
Dr.
University Medical Centre Ljubljana
Leiden, Slovenia
Marcel Beijk
Dr.
Amsterdam Medical Center, Netherlands
Lieuwe Piers
Dr.
Rijnstate Hospital, Netherlands
Henry Seligman, MD, MA
Dr.
National Heart and Lung Institute, Imperial College London, United Kingdom
Juan Iglesias
Dr.
Geneva University Hospitals, Switzerland
Arnoud 't Hof
Prof. Dr.
Maastricht University Medical Center, Netherlands
Erik Lipsic
Dr.
University Medical Center Groningen, Netherlands
Pairoj Chattranukulchai, MD, MSc
Dr.
King Chulalongkorn Memorial Hospital, Thailand

José Rodríguez-Palomares, MD, PhD, FSCMR
Prof. Dr.
Hospital Vall d'Hebron
Barcelona, Catalonia, Spain
Johannes Rigger
Dr.
Kantonsspital St. Gallen, Switzerland
Martijn Meuwissen
Dr.
Amphia Hospital, Netherlands
Lennaert Kleijn
Dr.
Treant Hospital, Netherlands
Bruno Pereira
Dr.
Institut National de Chirurgie Cardiaque et Cardiologie Invasive, Luxembourg

Lorenzo Monti, MD
Cardio-radiologist, Head Radiology Unit
ICS Maugeri Pavia
Pavia, Lombardia, Italy
René van der Schaaf, MD, PhD
Dr.
Onze Lieve Vrouwe Gasthuis Amsterdam, Netherlands
Juan Sanchis
Dr.
INCLIVA Health Research Institute, Spain
Guido Belli
Dr.
Clinica Polispecialistica San Carlo, Milan, Italy

Raymond Kim, MD
Professor
Duke Cardiovascular Magnetic Resonance Center
Durham, North Carolina, United States
Jan Tijssen, PhD
Prof.
Amsterdam Medical Center, Netherlands
Troels Thim
Dr.
Aarhus University Hospital, Denmark
Niels van Royen, MD, PhD
Prof. Dr.
Radboud University Medical Center, Netherlands
The preferred timing of treatment of nonculprit lesions in patients with ST-segment elevation myocardial infarction (STEMI) remains uncertain. A comparison of immediate percutaneous coronary intervention (PCI) guided by instantaneous wave-free ratio (iFR) versus deferred PCI guided by stress cardiac magnetic resonance imaging (CMR) in patients with STEMI and multivessel disease is warranted.
Methods:
In this international, investigator-initiated, open-label, randomized, controlled trial, patients with STEMI and at least one nonculprit lesion who had undergone successful primary PCI were randomly assigned in a 1:1 ratio to immediate iFR-guided PCI (in lesions with >50% stenosis and an iFR of ≤0.89 [normal, >0.89]) or deferred cardiac stress CMR–guided PCI within 6 weeks after randomization. The primary end point was a composite of death from any cause, recurrent myocardial infarction, or hospitalization for heart failure at 3-year follow-up.
Results:
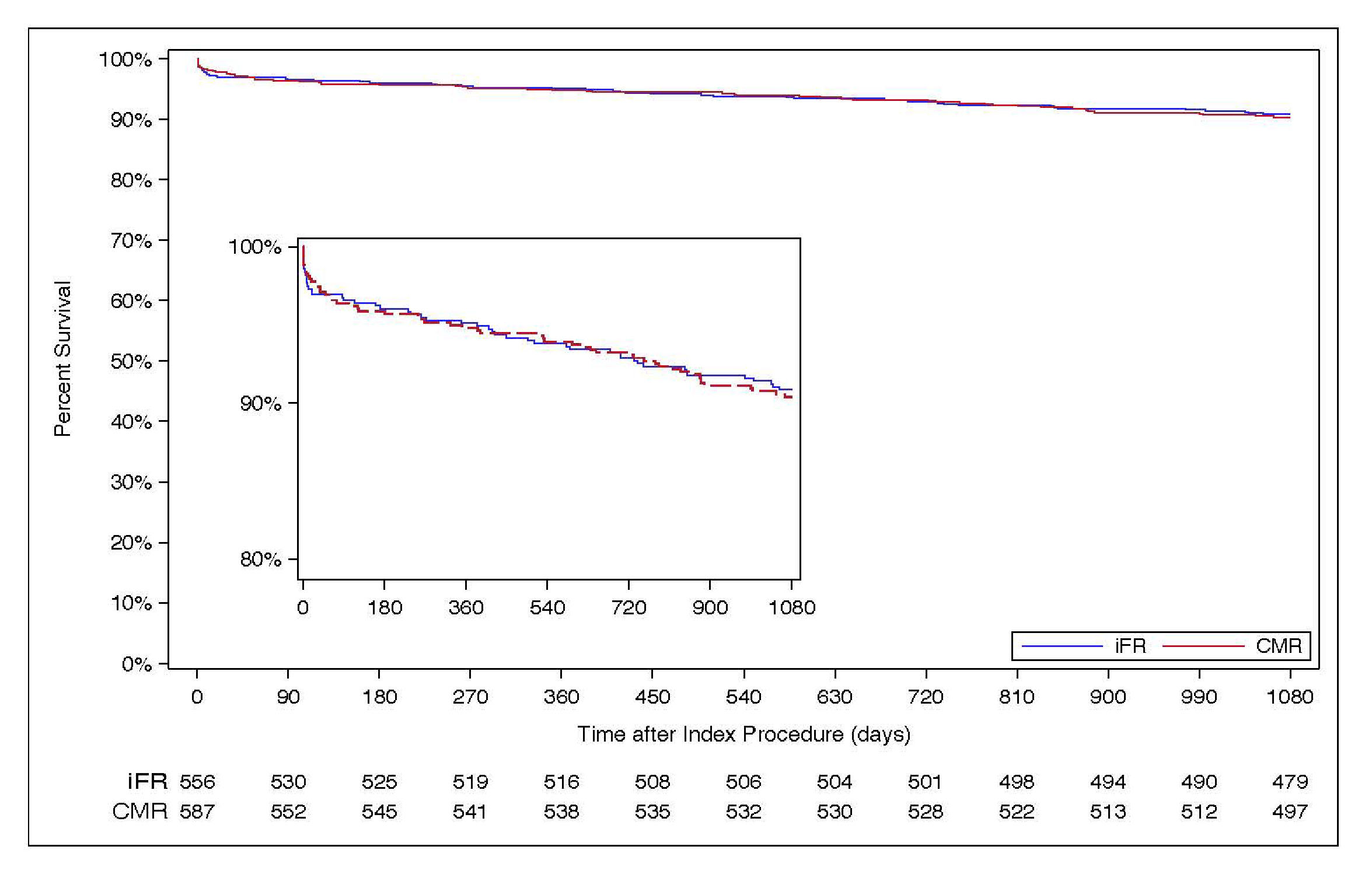
The trial included 1146 patients (558 in the iFR group and 588 in the CMR group) with a mean (±SD) age of 63±11 years; 78% were men. A total of 237 of 556 patients (42.6%) in the iFR group and 110 of 587 patients (18.7%) in the CMR group underwent PCI of nonculprit coronary arteries. A primary end-point event occurred in 50 patients (9.3%) in the iFR group and in 55 patients (9.8%) in the CMR group (hazard ratio, 0.95; 95% confidence interval, 0.65 to 1.40; P = 0.81). Serious adverse events occurred in 145 patients in the iFR group and in 181 in the CMR group.
Conclusion:
Among patients with STEMI who have undergone primary PCI, immediate iFR-guided PCI was not superior to deferred stress CMR-guided PCI of nonculprit coronary-artery lesions with respect to death from any cause, recurrent myocardial infarction, or hospitalization for heart failure at 3 years.
Kaplan-Meier Plot of Event-Free Survival