Rapid Fire Session

Luuk H.G.A Hopman, PhD
Postdoctoral Researcher Cardiology
Amsterdam UMC
Amsterdam, Noord-Holland, Netherlands
Luuk H.G.A Hopman, PhD
Postdoctoral Researcher Cardiology
Amsterdam UMC
Amsterdam, Noord-Holland, Netherlands
Nikki van Pouderoijen, MSc
PhD Student
Amsterdam UMC, Netherlands
Marisa van der Graaf
MD
St. Antonius Hospital Nieuwegein, Netherlands
Bob Abeln
MD
St. Antonius Hospital Nieuwegein, Netherlands
Michiel J.B. Kemme, MD, PhD
Cardiologist-Electrophysiologist
Amsterdam Medical Center, Netherlands
Max Liebregts
MD, PhD
St. Antonius Hospital Nieuwegein, Netherlands
Lucas Boersma
MD, PhD
St. Antonius Hospital Nieuwegein, Netherlands

Cor P. Allaart, MD, PhD
Cardiologist
Amsterdam Medical Center
Amsterdam, Noord-Holland, Netherlands
Marco J.W Götte, MD, PhD
MD, PhD
Stephenson Cardiac Imaging Centre
Calgary, Alberta, Canada
Year | Ablation modality | Scanner | LGE quantification | Most important CMR findings | |||
McGann et al. | 2008 | RF point-by-point1 (n= 46) | 1.5Ta
| Software: OsiriX & Matlab Analysis: LGE defined as a voxel intensity of 3 SD above normal/healthy tissue mean pixel intensity. | LA scar burden: PVI non-responders: 12.4 ± 5.7% PVI responders: 19.3 ± 6.7% | ||
Halbfass et al. | 2014 | Cryoballoon2 (n= 30) | 3.0Tb | Software: Corview Analysis: LGE is identified with a normalized voxel intensity. | Ratio of circumferentially encircled PVs: 33% Complete circumferential ablation lesions: 62% of left PVs vs. 7% of right PVs (p < 0.001) | ||
Akoum et al. | 2015 | RF point-by-point1 (n= 157) Cryoballoon2 (n= 12) RF single-shot3 (n= 8) | Both 1.5T and 3.0Tf
| Software: Corview Analysis: LGE defined as a voxel intensity of 2 SD above normal/healthy tissue mean pixel intensity.
| Procedure: PVI-only n= 111 (62.7%); PVI + additional ablation n= 52 (29.4%) Other n= 14 (7.9%) LA scar burden: Overall: 10.7 ± 4.9% PVI-only group: RF: 10.5 ± 4.3% Cryoballoon: 13.4 ± 6.2% RF PVAC: 7.1 ± 2.3% Ratio of circumferentially encircled PVs: 7.3% | ||
Khurram et al. | 2015 | RF point-by-point1 (n= 7) Cryoballoon4 (n= 5) | 1.5Ta
| Software: OsiriX and QMass MR Analysis: LGE quantified based on the IIR relative to the blood pool, threshold of ≥0.97. | LA scar burden: RF: 46.3 ± 3.6% (pre-ablation: 29.0 ± 6.8%) Cryoballoon: 50.0 ± 8.6% (pre-ablation: 38.0 ± 10.7%) | ||
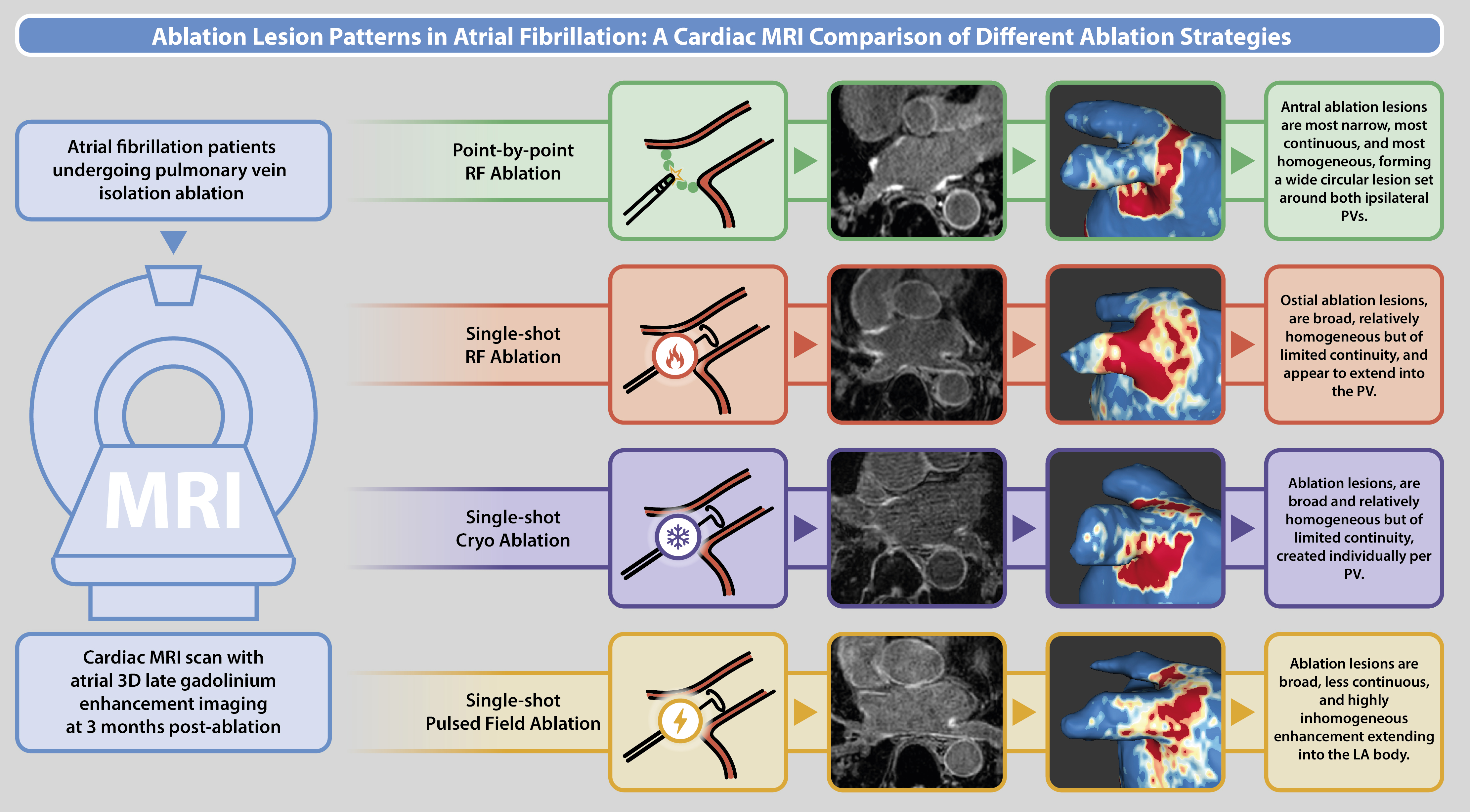
Jefairi et al. | 2018 | RF single-shot5 (n= 23) RF point-by-point1 (n= 28) | 1.5Ta | Software: MUSIC Analysis: LGE defined as a threshold of 50-70% of maximum signal intensity. | PV scar burden: 7.8 ± 2.1 mL, higher in patients treated with the RF single-shot catheter (8.6 ± 1.7 mL vs. 7.1 ± 2.2 mL) Gaps in scar formation around PVs were found in: 76% of patients (single-shot: 65% vs. point-by-point: 86%) 39% of PVs (single-shot: 41% vs. point-by-point: 56%) | ||
Kurose et al. | 2020 | RF point-by-point6 (n= 12) Cryoballoon2 (n= 18) | 1.5Tc | Software: Ziostation Analysis: LGE defined as a voxel intensity of 2 SD above normal/healthy tissue mean pixel intensity. NB: CMR performed 1-3 months | Lesion width and total number of gaps in scar formation: RF 6.3 ± 2.2mm; gaps 13% Cryoballoon: 8.1 ± 2.2mm; gaps 22% | ||
Nakatani et al. | 2021 | PFA7 (n= 18) RF point-by-point1 (n= 7) Cryoballoon2 (n= 16) | 1.5Td | Software: MUSIC Analysis: FWHM, the maximum signal intensity as an internal reference and a threshold set at 50% maximum intensity. | No discrete values of scar at 3 months but reversibility of 60% for PFA and 18% for thermal as compared to MRI within 3 hours post-PVI. | ||
Nelson et al. | 2022 | RF point-by-point1 (n= 313) Cryoballoon2 (n= 51) | 1.5Tf | Software: Merisight Analysis: LGE defined as a voxel intensity of 2-4 SD above normal/healthy tissue mean pixel intensity.
| LA scar burden: RF 8.8 ± 4.2% Cryoballoon 6.4 ± 3.6% | ||
Regany et al. | 2023 | RF point-by-point1 (n= 47) Cryoballoon2 (n= 40) | 3.0Te | Software: ADAS 3D Analysis: LGE quantified based on the IIR relative to the blood pool, threshold of >1.2. | Ratio of circumferentially encircled PVs and number of gaps in isolation per patient: RF: 39%, gaps: 2.7 Cryoballoon: 24%, gaps: 3.2 | ||
Sohns et al.
| 2023 | PFA7 (n= 10) | Not reported
| Software: Merisight Analysis: LGE defined as a voxel intensity of 2-4 SD above normal/healthy tissue mean pixel intensity. | Procedure: PVI and posterior wall isolation: LA scar burden: 8.1 ± 2.1% Mean scar width: 12.8 ± 2.1mm Bilateral PV encirclement: 37 out of 40 PVs (92.7%) | ||
Sciacca et al. | 2023 | vHPSD RF point-by-point8 (n= 30) | 3.0Tc | Software: Merisight Analysis: LGE defined as a voxel intensity of 2-4 SD above normal/healthy tissue mean pixel intensity. | LA scar burden: 9.5 ± 1.9% Mean scar width: 13.6 ± 2.9mm Gaps in scar formation around PVs: 10 patients (33.3%), mean 1.8 ± 1 gap/patient | ||
Fink et al.
| 2025 | PFA9 (n= 20) | Not reported
| Software: Merisight Analysis: LGE defined as a voxel intensity of 2-4 SD above normal/healthy tissue mean pixel intensity. | Bilateral PV encirclement: 16 patients (80%) LA scar burden: 6.1 ± 1.9% Mean scar width: left PVs 12.1 ± 3.1mm; right PVs: 10.7 ± 2.3mm. | ||
Regany‑Closa et al. | 2025 | RF point-by-point1 (n= 43) vHPSD RF point-by-point8 (n= 25) Cryoballoon2 (n= 40) PFA7 (n= 30) | 3.0Te
| Software: ADAS 3D Analysis: LGE quantified based on the IIR relative to the blood pool, threshold of ≥1.2.
| Ratio of circumferentially encircled PVs and mean lesion width: RF: 26%, lesion width: 8.7 mm vHPSD: 40%, lesion width: 10.9 mm Cryoballoon: 24%, lesion width: 13.3 mm PFA: 12%, lesion width: 12.7 mm | ||
Abbreviations: CMR, cardiac magnetic resonance; FWHM, full-width half-max; IIR, image intensity ratio; PV, pulmonary vein; PVI, pulmonary vein isolation; others as reported in previous tables. | Ablation modality 1THERMOCOOL SMARTTOUCH/NAVISTAR, Biosense Webster 2 ArcticFront (Advance), Medtronic 3PVAC, Medtronic 4Freezor MAX, Medtronic 5nMARQ, Biosense Webster 6TactiCath, Abbott 7FARAPULSE, Boston Scientific 8QDOT Micro, Biosense Webster 9VLC, Varipulse, Biosense Webster | Scanner aAVANTO, Siemens bVerio, Siemens cAchieva, Philips Medical dAERA, Siemens ePRISMA, Siemens
| |||||
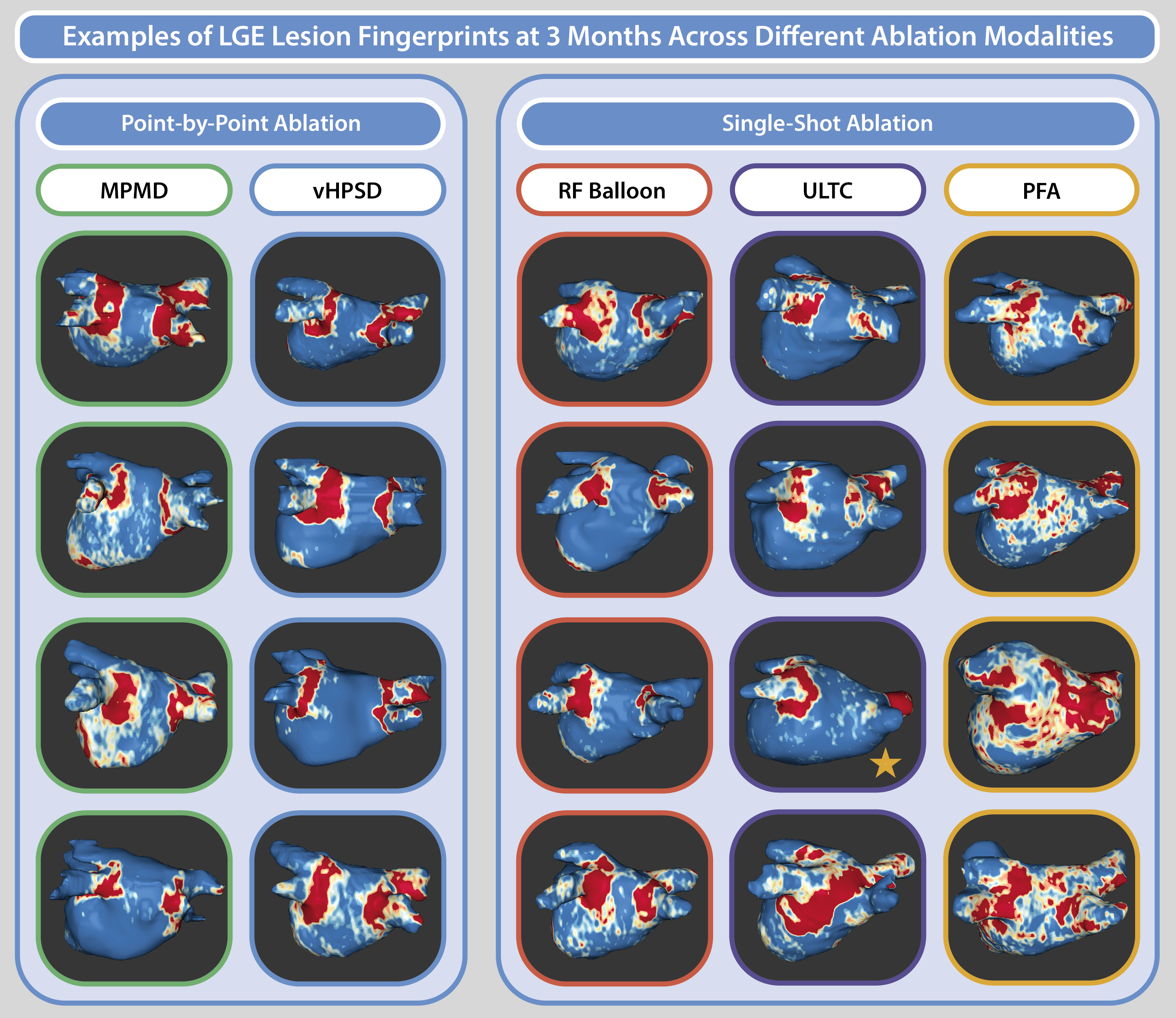
 LGE lesion fingerprints 3 months post-PVI across different ablation modalities
LGE lesion fingerprints 3 months post-PVI across different ablation modalities