Early Career Award Session
Virtual Recording
Congenital Track
Thara Nallamothu, BA
PhD Candidate
Northwestern University
Chicago, Illinois, United States
Thara Nallamothu, BA
PhD Candidate
Northwestern University
Chicago, Illinois, United States

Elizabeth Weiss, PhD
MD/PhD student
Northwestern University
Chicago, Illinois, United States
Justin Baraboo, MSc
PhD candidate
Northwestern University
Chicago, Illinois, United States

Joshua D. Robinson, MD, FSCMR
Section Head, Cardiac Imaging
Lurie Children's / Northwestern University
Chicago, Illinois, United States

Cynthia K. Rigsby, MD
Chair
Ann & Robert H. Lurie Children's Hospital of Chicago
Chicago, Illinois, United States
Matthias Stuber, PhD
Professor/Director
CIBM/CHUV/UNIL
Lausanne, Switzerland

Christopher W. Roy, PhD
Lecturer
University Hospital (CHUV) and University of Lausanne (UNIL)
Lausanne, Vaud, Switzerland
Michael Markl, PhD
Professor
Northwestern University Feinberg School of Medicine
Chicago, Illinois, United States
 Figure 2: Respiratory variability in KE, EL, and EL/KE, computed as the 100%*(max-min)/mean. a) KE: Fontan Adults (red) had increased respiratory variability in SVC (50%, p<0.05), IVC (74%, p<0.05), and PA KE (74%, p<0.01) compared to controls (gray, 15-29%). Fontan Peds (black) had increased respiratory variability in IVC KE (92%, p<0.01) compared to controls. Fontan Peds-GA (blue) had increased respiratory variability in SVC (55%, p<0.05) and PA KE (74%, p<0.05) compared to controls. b) EL: Fontan Peds-GA had increased respiratory variability in PA EL (63%, p<0.05) compared to controls (29%). c) EL/KE: Fontan Adults had increased respiratory variability in PA EL/KE (61% p<0.05) and decreased in aorta EL/KE (15% p<0.05) compared to controls (27-29%).
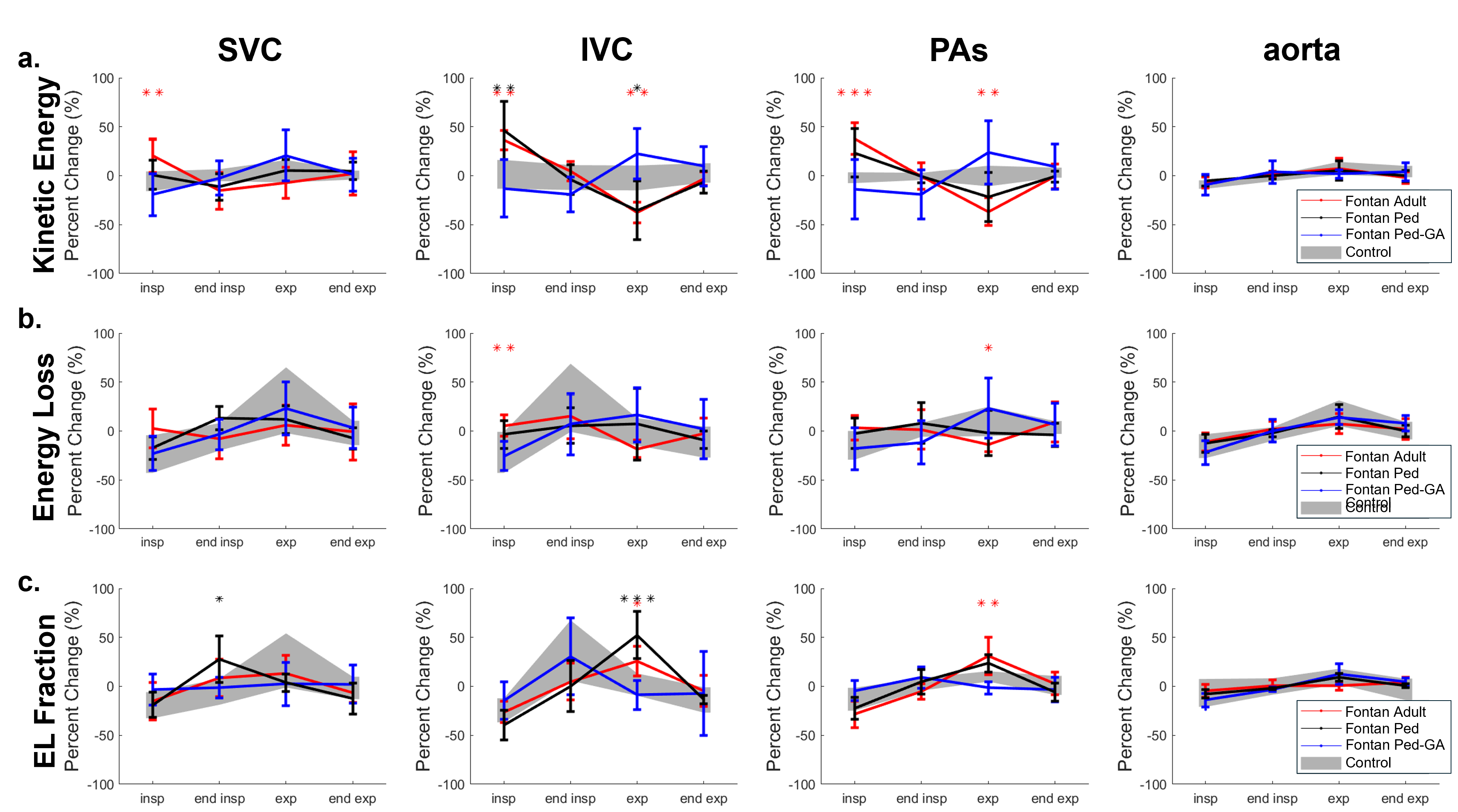
Figure 2: Respiratory variability in KE, EL, and EL/KE, computed as the 100%*(max-min)/mean. a) KE: Fontan Adults (red) had increased respiratory variability in SVC (50%, p<0.05), IVC (74%, p<0.05), and PA KE (74%, p<0.01) compared to controls (gray, 15-29%). Fontan Peds (black) had increased respiratory variability in IVC KE (92%, p<0.01) compared to controls. Fontan Peds-GA (blue) had increased respiratory variability in SVC (55%, p<0.05) and PA KE (74%, p<0.05) compared to controls. b) EL: Fontan Peds-GA had increased respiratory variability in PA EL (63%, p<0.05) compared to controls (29%). c) EL/KE: Fontan Adults had increased respiratory variability in PA EL/KE (61% p<0.05) and decreased in aorta EL/KE (15% p<0.05) compared to controls (27-29%)..png) Figure 3: Alterations in respiratory-driven dynamics in KE, EL, and EL/KE. For each respiratory phase, the % change in each metric relative to the mean over all respiratory phases was computed. Tukey tests were performed following . Repeated measures ANOVAs. a) KE: Fontan Adults (red) had increased inspiratory KE in SVC (+20% vs. -6%, p<0.01), IVC (+36% vs. +1%, p<0.01), and PAs (+38% vs. -2%, p<0.001), and decreased expiratory KE in IVC (-38% vs. -2%, p<0.01) and PAs (-36% vs. -0.3%, p<0.01) compared to controls (gray). Fontan Peds (black) had increased inspiratory IVC KE (+46%, p<0.01) and decreased expiratory IVC KE (-35%, p<0.05) compared to controls. b) EL: Fontan Adults had increased inspiratory IVC EL (+5% vs. -21%, p<0.01) and decreased expiratory PA EL (-14% vs. +8%, p<0.05) compared to controls. c) EL/KE: Fontan Adults and Peds had increased expiratory IVC EL/KE (+26%, +52% vs. +2%, p<0.05, p<0.001). Fontan adults had increased expiratory PA EL/KE (+31% vs. +10%, p<0.01).
Figure 3: Alterations in respiratory-driven dynamics in KE, EL, and EL/KE. For each respiratory phase, the % change in each metric relative to the mean over all respiratory phases was computed. Tukey tests were performed following . Repeated measures ANOVAs. a) KE: Fontan Adults (red) had increased inspiratory KE in SVC (+20% vs. -6%, p<0.01), IVC (+36% vs. +1%, p<0.01), and PAs (+38% vs. -2%, p<0.001), and decreased expiratory KE in IVC (-38% vs. -2%, p<0.01) and PAs (-36% vs. -0.3%, p<0.01) compared to controls (gray). Fontan Peds (black) had increased inspiratory IVC KE (+46%, p<0.01) and decreased expiratory IVC KE (-35%, p<0.05) compared to controls. b) EL: Fontan Adults had increased inspiratory IVC EL (+5% vs. -21%, p<0.01) and decreased expiratory PA EL (-14% vs. +8%, p<0.05) compared to controls. c) EL/KE: Fontan Adults and Peds had increased expiratory IVC EL/KE (+26%, +52% vs. +2%, p<0.05, p<0.001). Fontan adults had increased expiratory PA EL/KE (+31% vs. +10%, p<0.01).