Innovations Track

M. Berk Sahin
PhD student
Purdue University
West Lafayette, Indiana, United States
M. Berk Sahin
PhD student
Purdue University
West Lafayette, Indiana, United States
Dilek M. Yalcinkaya, MSc
PhD Candidate
Purdue University
West Lafayette, Indiana, United States

Hazar Benan Unal, PhD
Postdoctoral Research Associate
Laboratory for Translational Imaging of Microcirculation, Purdue University
Indianapolis, Indiana, United States

Khalid Youssef, PhD, MSc
Assistant Professor
Indiana University, Department of Radiology and Imaging Sciences
Indianapolis, Indiana, United States
Abolfazl Hashemi, PhD, MSc, BSc
Assistant Professor
Purdue University, Indiana, United States
Behzad Sharif, PhD
Associate Professor
Purdue University
Indianapolis, Indiana, United States
.png) Figure 2: (A) Myocardial perfusion representative reconstruction results from two different scans of the same patient under no dataset shift and dataset shift due to a low-dose contrast protocol, highlighting the importance of using localized error metric to accurately assess the impact of dataset shift. From left to right, the first column shows the artifact-free scanner reconstruction, which is considered reference image. Subsequent columns display reconstructions from retrospectively subsampled data at effective acceleration rate of 3.5 using a Cartesian sampling with 10% calibration lines. These include a zero-filled reconstruction (inverse FFT with missing data set to zero), GRAPPA [5], and two DL-based methods (2D-static and 2D+time VarNet). Global (green) and localized (red) NRMSE values are shown at the top-left and top-right of each reconstruction. Under the low-dose protocol, global NRMSE increased by 0.4% for 2D-static and 0.1% for 2D+time reconstructions, while localized NRMSE increased by 4.7% and 3.6%, respectively. (B) Myocardial perfusion representative y-t cuts corresponding to the scans in (A). The first column shows the x-y view of the reference image with the cardiac region (red box) generated by a pre-trained localizer. Green dashed lines show the y-t cut location whereas red dashed lines follow the localization box on y-t cut over time. Global NRMSE was calculated over the full y–t cut, whereas localized NRMSE was calculated only within the segment of the y–t cut that falls inside the red box. Under the low-dose protocol dataset shift, global (green, top-left) NRMSE changed by 0.3% for 2D-static and 0.7% for 2D+time reconstructions, while localized NRMSE changed by 3.4% and 3.1%, respectively.
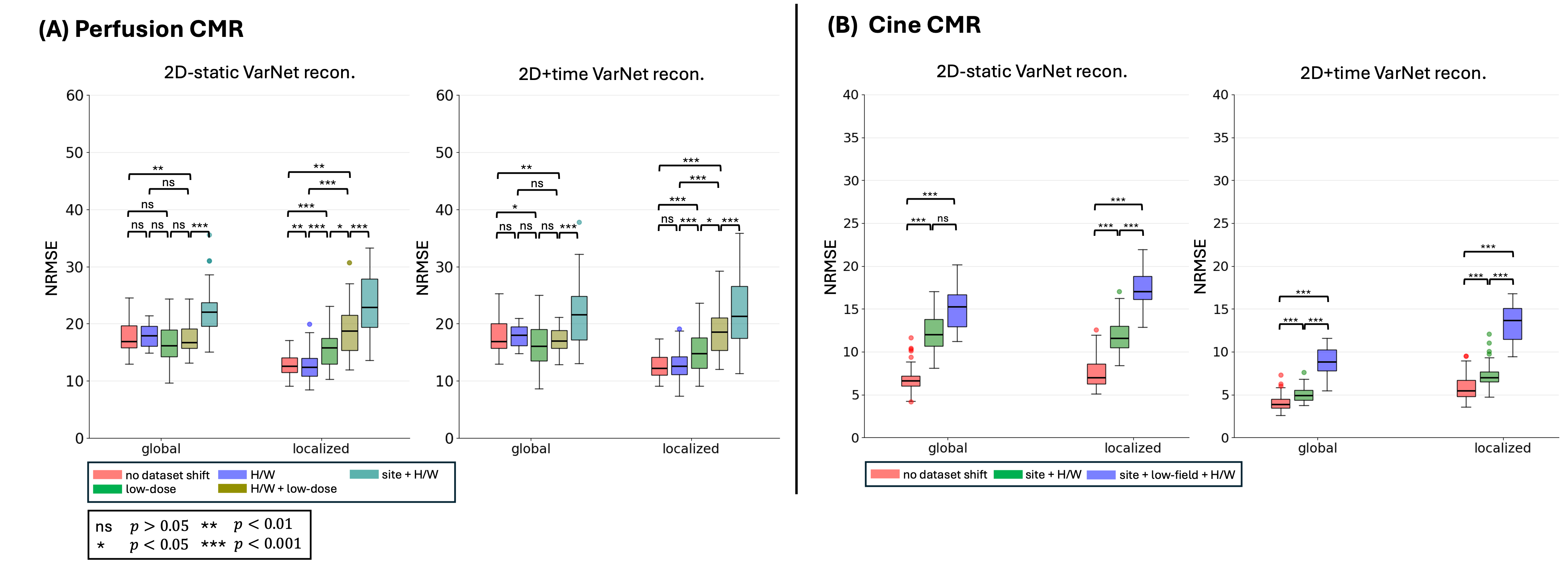
Figure 2: (A) Myocardial perfusion representative reconstruction results from two different scans of the same patient under no dataset shift and dataset shift due to a low-dose contrast protocol, highlighting the importance of using localized error metric to accurately assess the impact of dataset shift. From left to right, the first column shows the artifact-free scanner reconstruction, which is considered reference image. Subsequent columns display reconstructions from retrospectively subsampled data at effective acceleration rate of 3.5 using a Cartesian sampling with 10% calibration lines. These include a zero-filled reconstruction (inverse FFT with missing data set to zero), GRAPPA [5], and two DL-based methods (2D-static and 2D+time VarNet). Global (green) and localized (red) NRMSE values are shown at the top-left and top-right of each reconstruction. Under the low-dose protocol, global NRMSE increased by 0.4% for 2D-static and 0.1% for 2D+time reconstructions, while localized NRMSE increased by 4.7% and 3.6%, respectively. (B) Myocardial perfusion representative y-t cuts corresponding to the scans in (A). The first column shows the x-y view of the reference image with the cardiac region (red box) generated by a pre-trained localizer. Green dashed lines show the y-t cut location whereas red dashed lines follow the localization box on y-t cut over time. Global NRMSE was calculated over the full y–t cut, whereas localized NRMSE was calculated only within the segment of the y–t cut that falls inside the red box. Under the low-dose protocol dataset shift, global (green, top-left) NRMSE changed by 0.3% for 2D-static and 0.7% for 2D+time reconstructions, while localized NRMSE changed by 3.4% and 3.1%, respectively.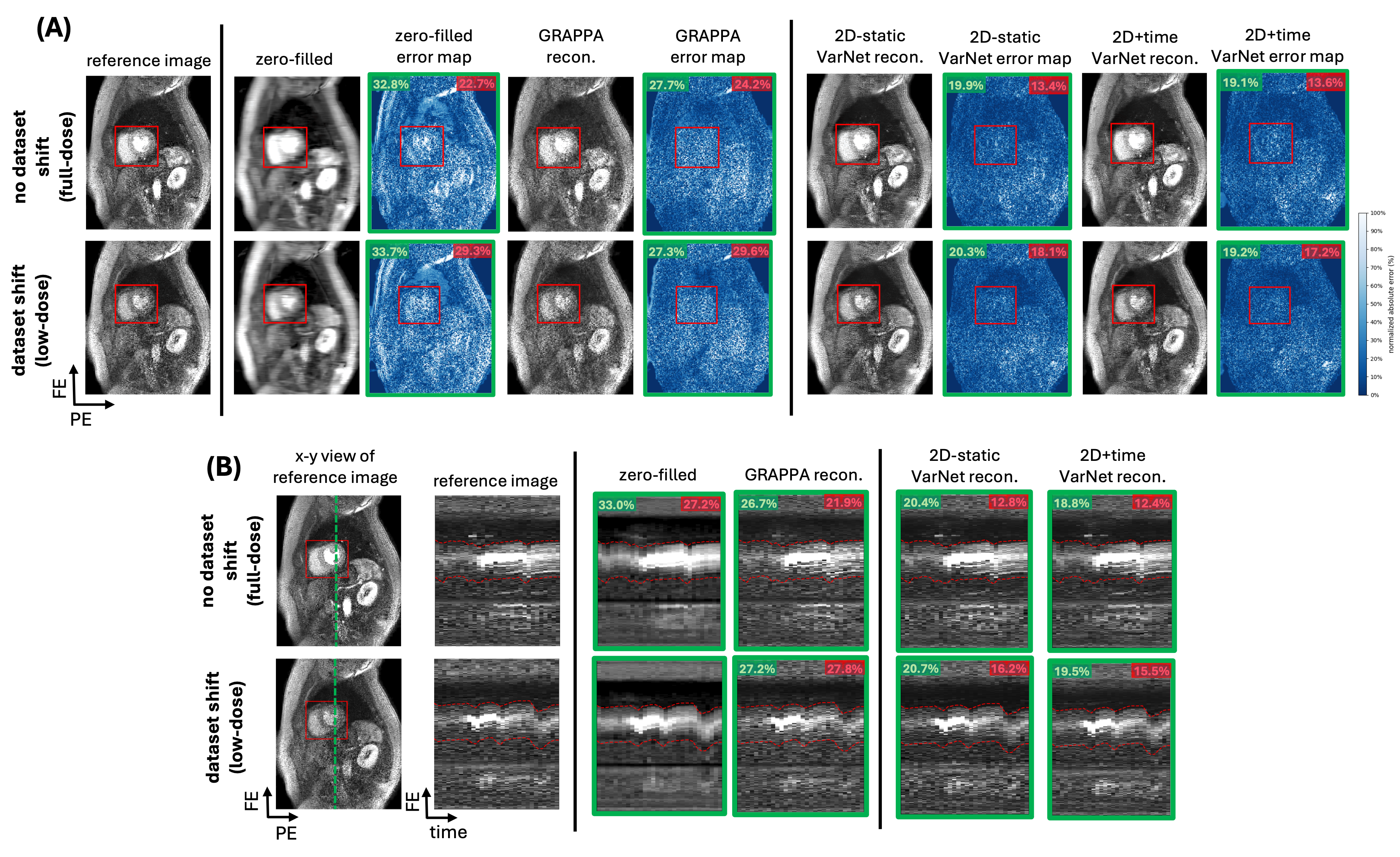 Figure 3: DL-based cardiac perfusion and cine reconstructions under different dataset shifts, illustrating that localized errors capture model generalization more effectively than global errors. Panels (A) and (B) show cumulative reconstruction results for perfusion and cine CMR at effective acceleration of 3.5 retrospectively, for two DL-based methods (2D-static and 2D+time VarNet), trained separately and evaluated on different test sets including “no dataset shift” case from Fig. 2B. Global NRMSE, computed over the entire image, shows little variation across test sets and statistically not significant (p>0.05). In contrast, localized NRMSE, computed within the cardiac region from the DL-based localizer, consistently separates the reconstruction error in different test sets and yields more statistically significant differences. This pattern is observed consistently across both DL models and both imaging modalities, demonstrating that localized NRMSE is more sensitive to dataset shifts than global NRMSE.
Figure 3: DL-based cardiac perfusion and cine reconstructions under different dataset shifts, illustrating that localized errors capture model generalization more effectively than global errors. Panels (A) and (B) show cumulative reconstruction results for perfusion and cine CMR at effective acceleration of 3.5 retrospectively, for two DL-based methods (2D-static and 2D+time VarNet), trained separately and evaluated on different test sets including “no dataset shift” case from Fig. 2B. Global NRMSE, computed over the entire image, shows little variation across test sets and statistically not significant (p>0.05). In contrast, localized NRMSE, computed within the cardiac region from the DL-based localizer, consistently separates the reconstruction error in different test sets and yields more statistically significant differences. This pattern is observed consistently across both DL models and both imaging modalities, demonstrating that localized NRMSE is more sensitive to dataset shifts than global NRMSE.