Quick Fire Session

Marwen Eid, MD
Cardiac Imaging Fellow
St. Francis Hospital, The Heart Center
Brooklyn , New York, United States
Giulia Passaniti, MD
Cardiac Imaging Fellow
St. Francis Hospital, The Heart Center
Roslyn, New York, United States
Amanda Leung, MD
Cardiologist
St. Francis Hospital, The Heart Center
Greenvale, New York, United States
Michaela Schmidt, RT
Siemens Healthcare GmbH, Erlangen, Germany
SIEMENS HEALTHCARE GmbH
Erlangen, Bayern, Germany

Rene M. Botnar
Professor of Cardiovascular Imaging
Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile
Santiago de Chile, Region Metropolitana, Chile

Claudia Prieto, PhD
Professor
Pontificia Universidad Católica de Chile / King's College London
Santiago, Region Metropolitana, Chile
Jason Craft, MD
Cardiologist
St. Francis Hospital, The Heart Center
Greenvale, New York, United States
 Fig 2- Demonstration of dual inferior venal cava anatomy using image-based navigator (iNAV) gadolinium enhanced MRA. (A) The azygos continuation joins the vertebral venous plexus (VVP), from which the left inferior vena cava (LIVC) originates. There is drainage of the left renal vein (LRV) into the LIVC. Inset- there is normal connection of the hemiazygos to the azygos vein. (B) Axial maximal intensity projection reformats demonstrate the relationship between the left renal artery (LRA), right renal artery (RRA), LIVC, and VVP. (C) The right renal vein (RRV) is a branch of the right inferior vena cava (RIVC), which terminates into the right atrium (RA). Notice continuation of the RIVC inferior to the origin of the RRV.
Fig 2- Demonstration of dual inferior venal cava anatomy using image-based navigator (iNAV) gadolinium enhanced MRA. (A) The azygos continuation joins the vertebral venous plexus (VVP), from which the left inferior vena cava (LIVC) originates. There is drainage of the left renal vein (LRV) into the LIVC. Inset- there is normal connection of the hemiazygos to the azygos vein. (B) Axial maximal intensity projection reformats demonstrate the relationship between the left renal artery (LRA), right renal artery (RRA), LIVC, and VVP. (C) The right renal vein (RRV) is a branch of the right inferior vena cava (RIVC), which terminates into the right atrium (RA). Notice continuation of the RIVC inferior to the origin of the RRV. 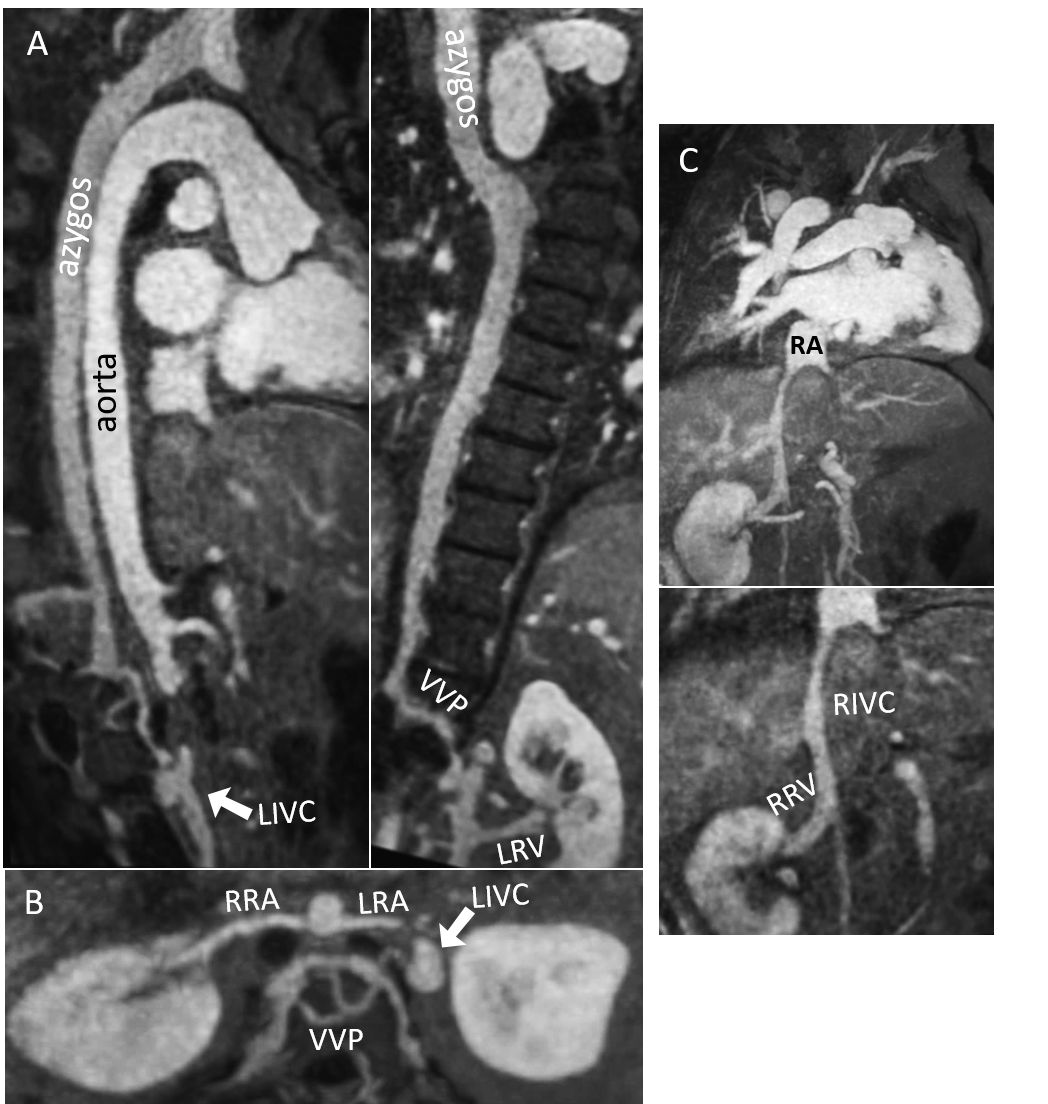 Fig 3- Twin curved multiplanar reformats from CTA imaging also demonstrated collateralization through the paraumbilical vein; proximal connection with the superficial epigastric vein (white arrow) and distal connection with the hepatic portal vein (black arrow).
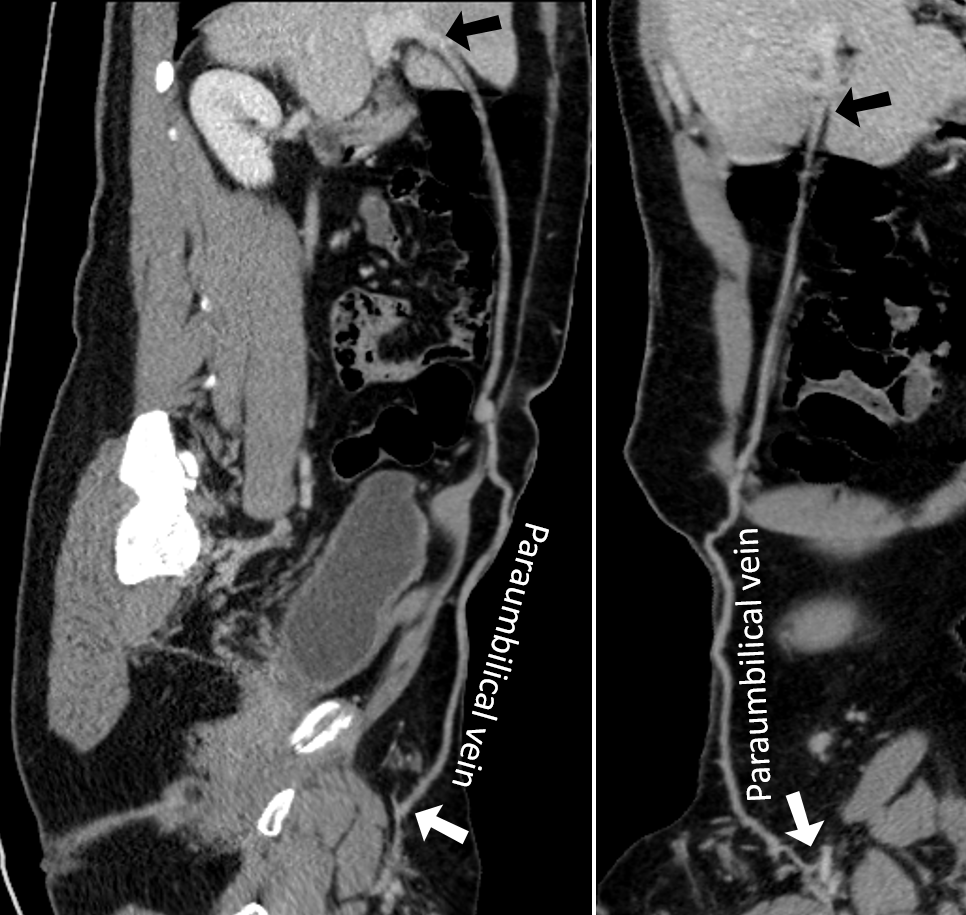
Fig 3- Twin curved multiplanar reformats from CTA imaging also demonstrated collateralization through the paraumbilical vein; proximal connection with the superficial epigastric vein (white arrow) and distal connection with the hepatic portal vein (black arrow).