Assistant professor Asahikawa Medical University Asahikawa, Hokkaido, Japan
Background: Right ventricular (RV) enlargement and elevated RV pressure caused by pulmonary valve regurgitation or stenosis can impair RV function and compress the left ventricle (LV), potentially affecting its mechanics. However, how RV-induced LV compression alters LV torsional mechanics and intracardiac flow remains poorly understood and warrants further investigation. We hypothesized that deformation of the LV, caused by RV overload, may influence LV torsional mechanics and alter intracardiac blood flow characteristics.
Methods: We studied 17 patients (age range: 12–37 years) with RV pressure or volume overload who underwent cardiac magnetic resonance imaging, along with 13 healthy controls (age range: 13–33 years). From cine images, we assessed LV torsion (deg/cm), twisting and untwisting torsion rates (deg/cm·s), and systolic and diastolic eccentricity indices. Additionally, 4D flow magnetic resonance imaging was used to analyze intracardiac flow components. This study was approved by the institutional review board.
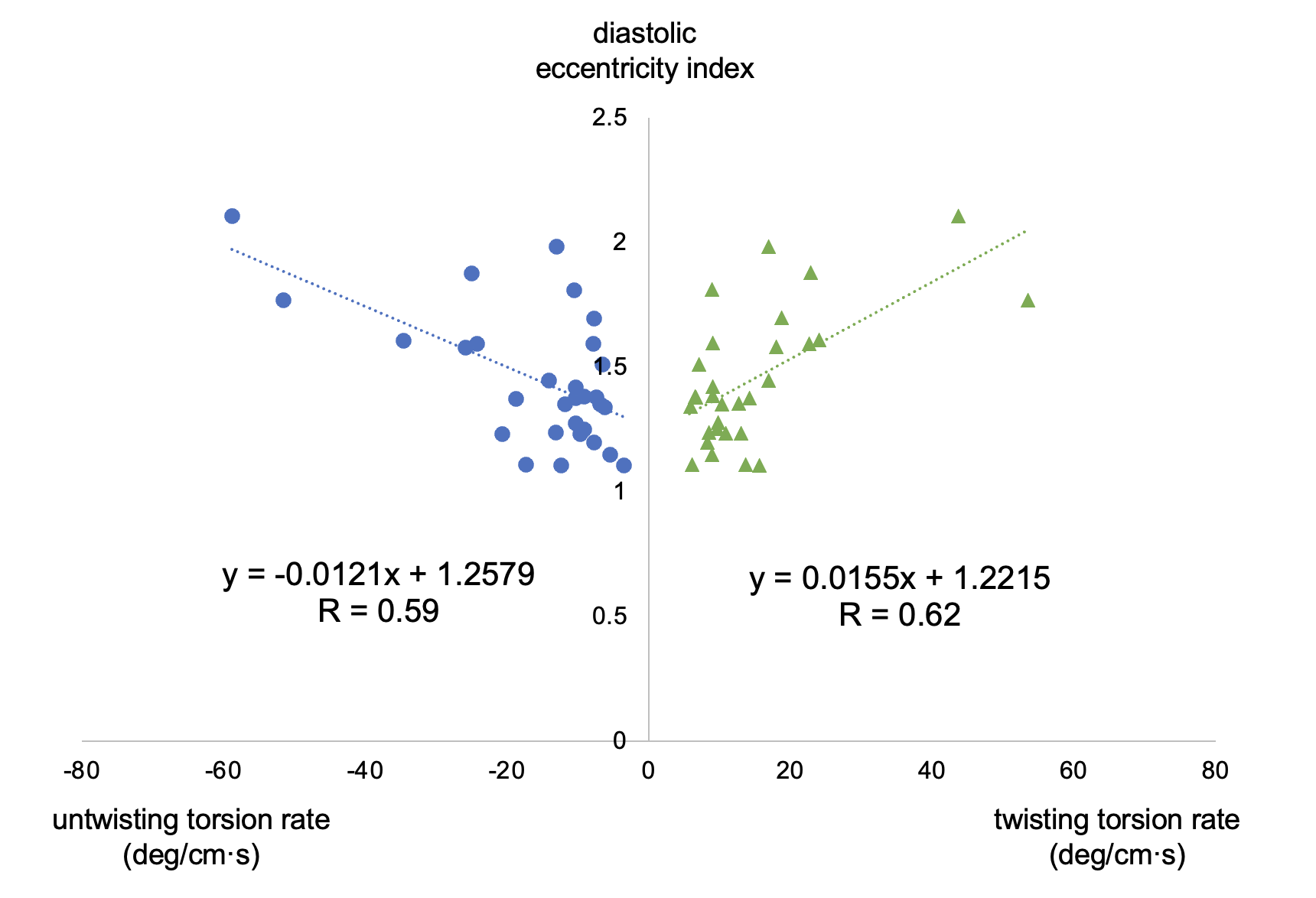
Results: Patients with RV overload showed significantly lower RVEF compared to controls (47.8 vs 53.1%, p = 0.014), while LVEF and LV global longitudinal strain (GLS) did not differ significantly (LVEF: 64.3 vs 65.3%, p = 0.509; GLS: −16.9 vs −16.4%, p = 0.363). LV torsion was similar between groups (1.0 vs 0.7 deg/cm, p = 0.563), but both twisting and untwisting torsion rates were significantly increased in the RV overload group (twisting torsion rate: 16.9 vs 9.6 deg/cm·s, p = 0.017; untwisting torsion rate: −13.2 vs −9.2 deg/cm·s, p = 0.007). Twisting and untwisting torsion rates were positively correlated with diastolic eccentricity index (twisting torsion rate: R = 0.62; untwisting torsion rate: R = 0.59), suggesting that increased LV deformation was associated with enhanced torsional activity. Twisting torsion rate also showed a positive correlation with delayed ejection flow, indicating altered intracardiac flow dynamics (R = 0.42). These results suggest that even in the absence of impaired LVEF or GLS, LV torsion rate and intracardiac flow are sensitive to structural deformation.
Conclusion: LV deformation caused by RV overload was associated with increased torsional motion and altered intracardiac flow composition. These parameters may serve as early indicators of subclinical LV dysfunction prior to changes in conventional metrics such as LVEF or GLS.
Twisting and untwisting torsion rates were positively correlated with diastolic eccentricity index (twisting torsion rate: R = 0.62; untwisting torsion rate: R = 0.59).