Rapid Fire Session
Dongyue Si, PhD
Research Associate
King's College London
London, England, United Kingdom
Dongyue Si, PhD
Research Associate
King's College London
London, England, United Kingdom

Simon J. Littlewood, MD
Clinical Research Fellow
King's College London
London, England, United Kingdom
Michael G. Crabb, PhD
Research Associate
King's College London
London, England, United Kingdom
.jpg "Karl P. Kunze, PhD photo")
Karl P. Kunze, PhD
Senior Cardiac MR Scientist
Siemens Healthineers
Camberley, England, United Kingdom

Claudia Prieto, PhD
Professor
Pontificia Universidad Católica de Chile / King's College London
Santiago, Region Metropolitana, Chile

Rene M. Botnar
Professor of Cardiovascular Imaging
Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile
Santiago de Chile, Region Metropolitana, Chile
 Figure 2. Representative images of a 66-year-old female patient acquired with different sequences. (A) LGE images acquired with 2D bright-blood PSIR, 2D grey-blood PSIR and 3D PSIR GB-BOOST in short-axis (SAX) and 2-chamber (2CH) views. The results showed negative LGE findings. 3D PSIR GB-BOOST had image contrast comparable with 2D grey-blood PSIR by nulling the signal of blood pool. (B) CMRA images acquired with 3D CMRA and 3D T2prep GB-BOOST with curved planar reconstruction to show left anterior descending artery (LAD) and right coronary artery (RCA) respectively. 3D T2prep GB-BOOST showed image contrast comparable with 3D CMRA, presenting good image quality for the depiction of the structure of both LAD and RCA.
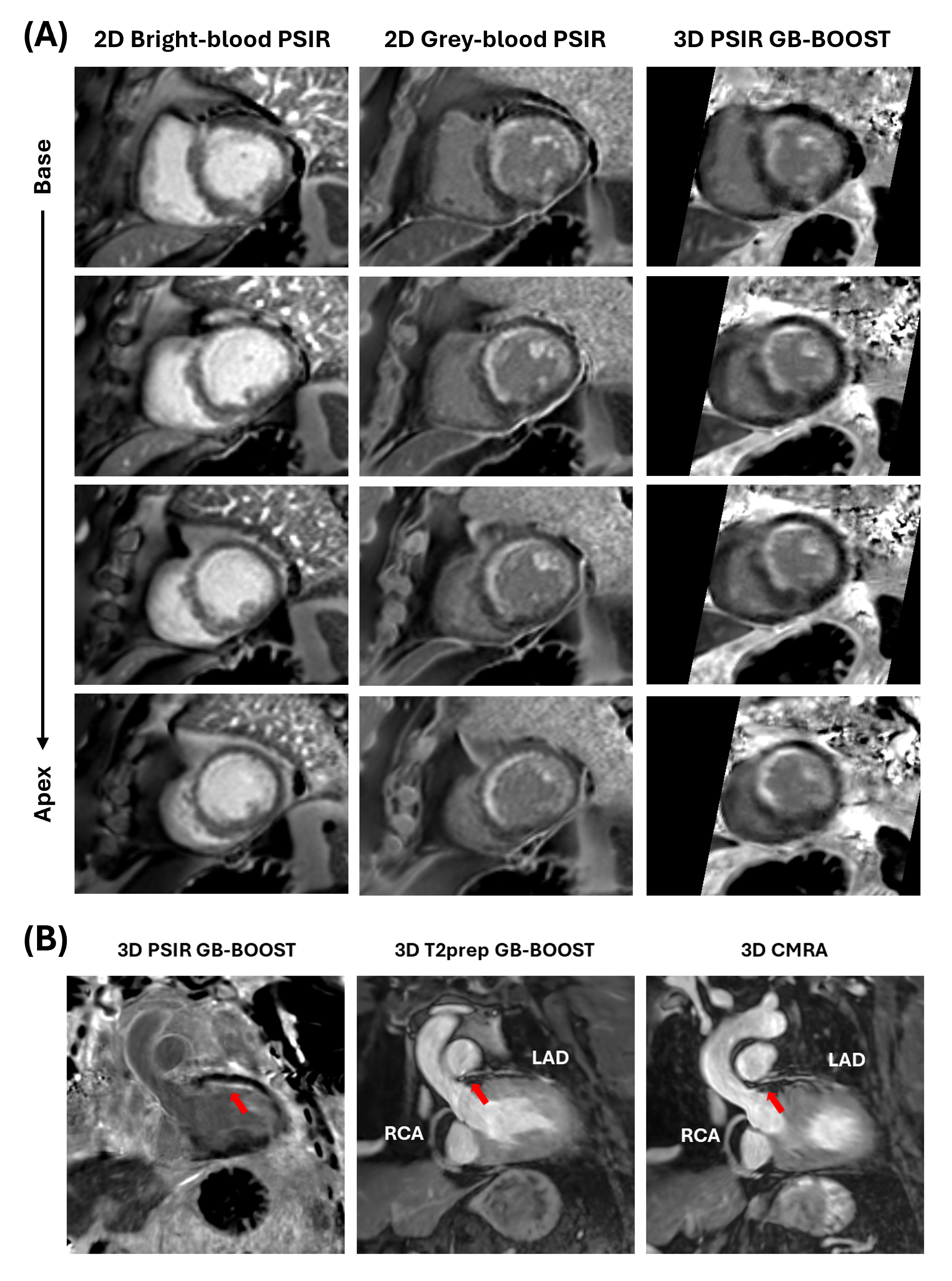
Figure 2. Representative images of a 66-year-old female patient acquired with different sequences. (A) LGE images acquired with 2D bright-blood PSIR, 2D grey-blood PSIR and 3D PSIR GB-BOOST in short-axis (SAX) and 2-chamber (2CH) views. The results showed negative LGE findings. 3D PSIR GB-BOOST had image contrast comparable with 2D grey-blood PSIR by nulling the signal of blood pool. (B) CMRA images acquired with 3D CMRA and 3D T2prep GB-BOOST with curved planar reconstruction to show left anterior descending artery (LAD) and right coronary artery (RCA) respectively. 3D T2prep GB-BOOST showed image contrast comparable with 3D CMRA, presenting good image quality for the depiction of the structure of both LAD and RCA.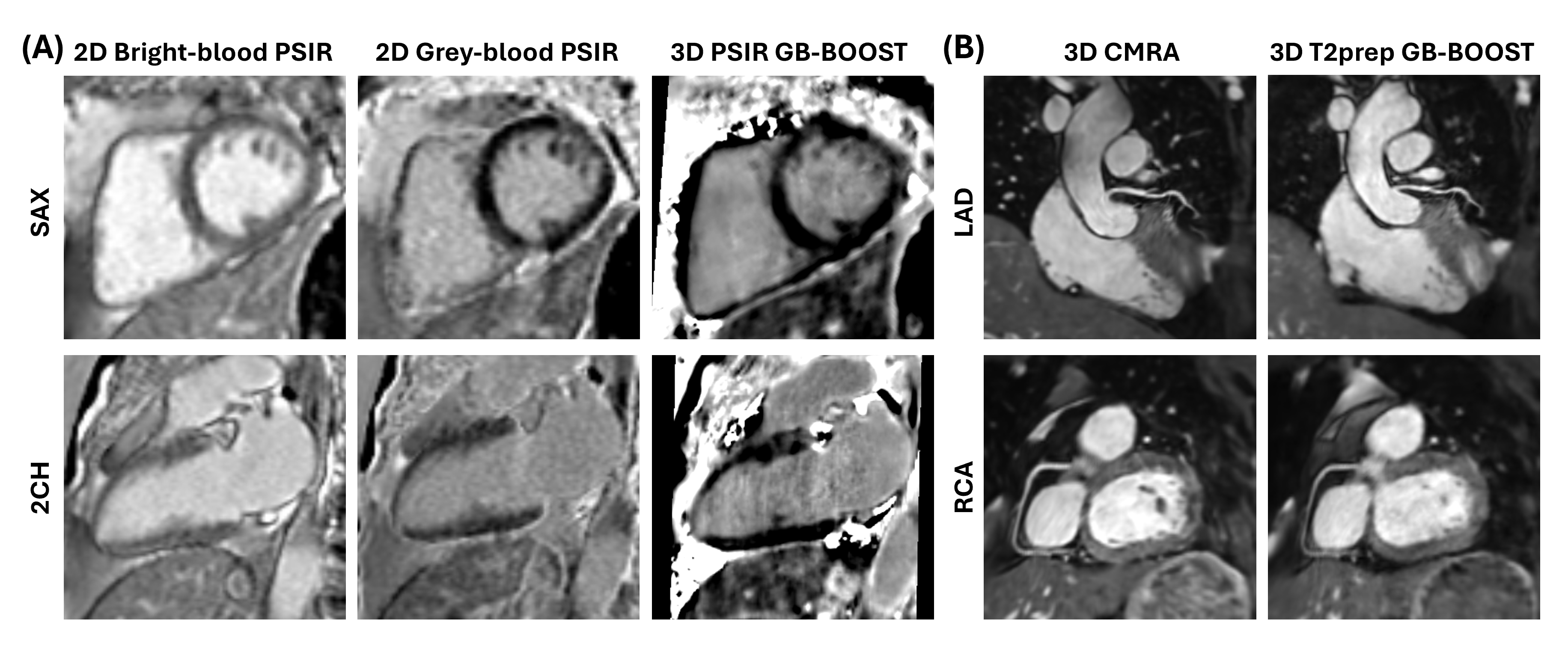 Figure 3. Images of a 74-year-old male patient with known left-ventricle impairment vsecondary to coronary artery disease with chronic total occlusion of left main coronary artery. (A) Short-axis LGE images acquired with 2D bright-blood PSIR, 2D grey-blood PSIR and 3D PSIR GB-BOOST. There was a large area of subendocardial myocardial infarction in the left anterior descending artery (LAD) and left circumflex territory. Bright-blood PSIR presented a poor contrast especially for the detection of subendocardial and papillary muscle enhancement, while 3D PSIR GB-BOOST and 2D grey-blood PSIR had superior contrast, presenting consistent findings regarding the scar area across the heart. (B) Curved planner reconstructions of 3D GB-BOOST and 3D CMRA of the same patient. The occlusion of left main coronary artery was confirmed by the 3D T2prep GB-BOOST and 3D CMRA images (red arrows). In addition, PSIR GB-BOOST image with the same curved planner reconstruction showed scar area highly correlated with the left main coronary artery territory (red arrow).
Figure 3. Images of a 74-year-old male patient with known left-ventricle impairment vsecondary to coronary artery disease with chronic total occlusion of left main coronary artery. (A) Short-axis LGE images acquired with 2D bright-blood PSIR, 2D grey-blood PSIR and 3D PSIR GB-BOOST. There was a large area of subendocardial myocardial infarction in the left anterior descending artery (LAD) and left circumflex territory. Bright-blood PSIR presented a poor contrast especially for the detection of subendocardial and papillary muscle enhancement, while 3D PSIR GB-BOOST and 2D grey-blood PSIR had superior contrast, presenting consistent findings regarding the scar area across the heart. (B) Curved planner reconstructions of 3D GB-BOOST and 3D CMRA of the same patient. The occlusion of left main coronary artery was confirmed by the 3D T2prep GB-BOOST and 3D CMRA images (red arrows). In addition, PSIR GB-BOOST image with the same curved planner reconstruction showed scar area highly correlated with the left main coronary artery territory (red arrow).