Early Career Award Session
Virtual Recording

Hazar Benan Unal, PhD
Postdoctoral Research Associate
Laboratory for Translational Imaging of Microcirculation, Purdue University
Indianapolis, Indiana, United States
Hazar Benan Unal, PhD
Postdoctoral Research Associate
Laboratory for Translational Imaging of Microcirculation, Purdue University
Indianapolis, Indiana, United States
Shahriar Zeynali, MSc
PhD Candidate
Indiana University School of Medicine
Indianapolis, Indiana, United States
Arian M. Sohi, BSc
PhD Student
Laboratory for Translational Imaging for Microcirculation, Weldon School of Biomedical Engineering, Purdue University
Indianapolis, Indiana, United States
Eric Anttila, PhD
Research Engineer
MED Institute, United States

Rohan Dharmakumar, PhD
Executive Director
Indiana University School of Medicine
Indianapolis, Indiana, United States

David Gross, PhD
Director of MRI Safety Evaluations and Engineering Simulations
MED Institute
West Lafayette, Indiana, United States
Behzad Sharif, PhD
Associate Professor
Purdue University
Indianapolis, Indiana, United States
 Figure 2. Example in vivo cases showing T1 maps, ferumoxytol-enhanced (FE) T1 reactivity, and MBV reserve (MBVR) in a healthy subject (top row) and one with varying degrees of microvascular disease (bottom row). (A) In the healthy subject, both FE T1 reactivity and MBVR appear relatively consistent throughout the myocardium, with expected physiological variations. (B) In the diseased subject, both metrics clearly distinguish between regions of severe ischemia (LAD), mild ischemia (LCX), and unaffected myocardium (RCA). Importantly, MBVR values in the RCA region remain comparable to those in the healthy case, underscoring its reliability as a physiological biomarker that is independent of dose. In contrast, FE T1 reactivity in the same RCA area shows noticeable differences (nearly −13% vs. −7%), likely reflecting variations in ferumoxytol dosage between the two experiments.
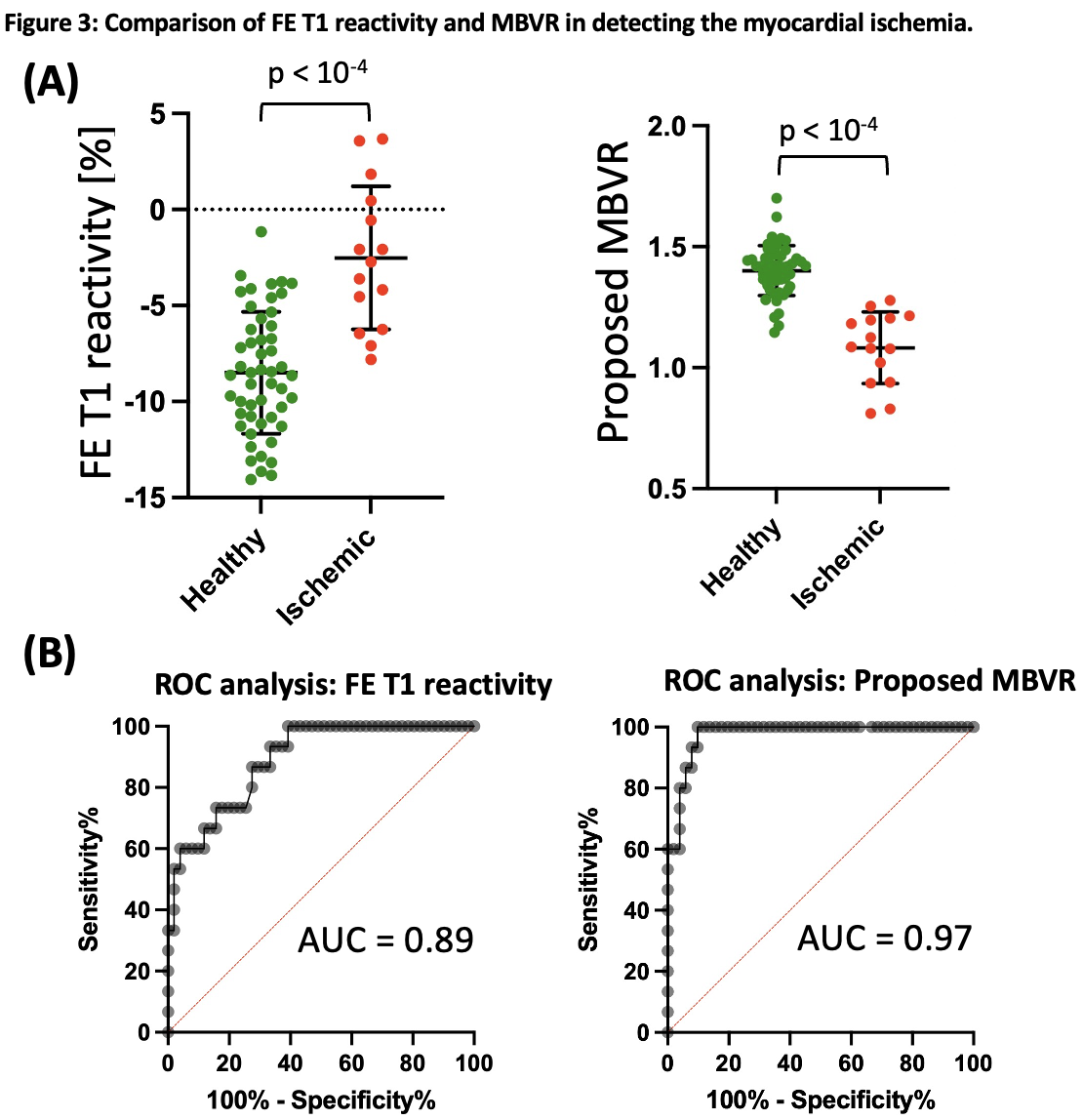
Figure 2. Example in vivo cases showing T1 maps, ferumoxytol-enhanced (FE) T1 reactivity, and MBV reserve (MBVR) in a healthy subject (top row) and one with varying degrees of microvascular disease (bottom row). (A) In the healthy subject, both FE T1 reactivity and MBVR appear relatively consistent throughout the myocardium, with expected physiological variations. (B) In the diseased subject, both metrics clearly distinguish between regions of severe ischemia (LAD), mild ischemia (LCX), and unaffected myocardium (RCA). Importantly, MBVR values in the RCA region remain comparable to those in the healthy case, underscoring its reliability as a physiological biomarker that is independent of dose. In contrast, FE T1 reactivity in the same RCA area shows noticeable differences (nearly −13% vs. −7%), likely reflecting variations in ferumoxytol dosage between the two experiments.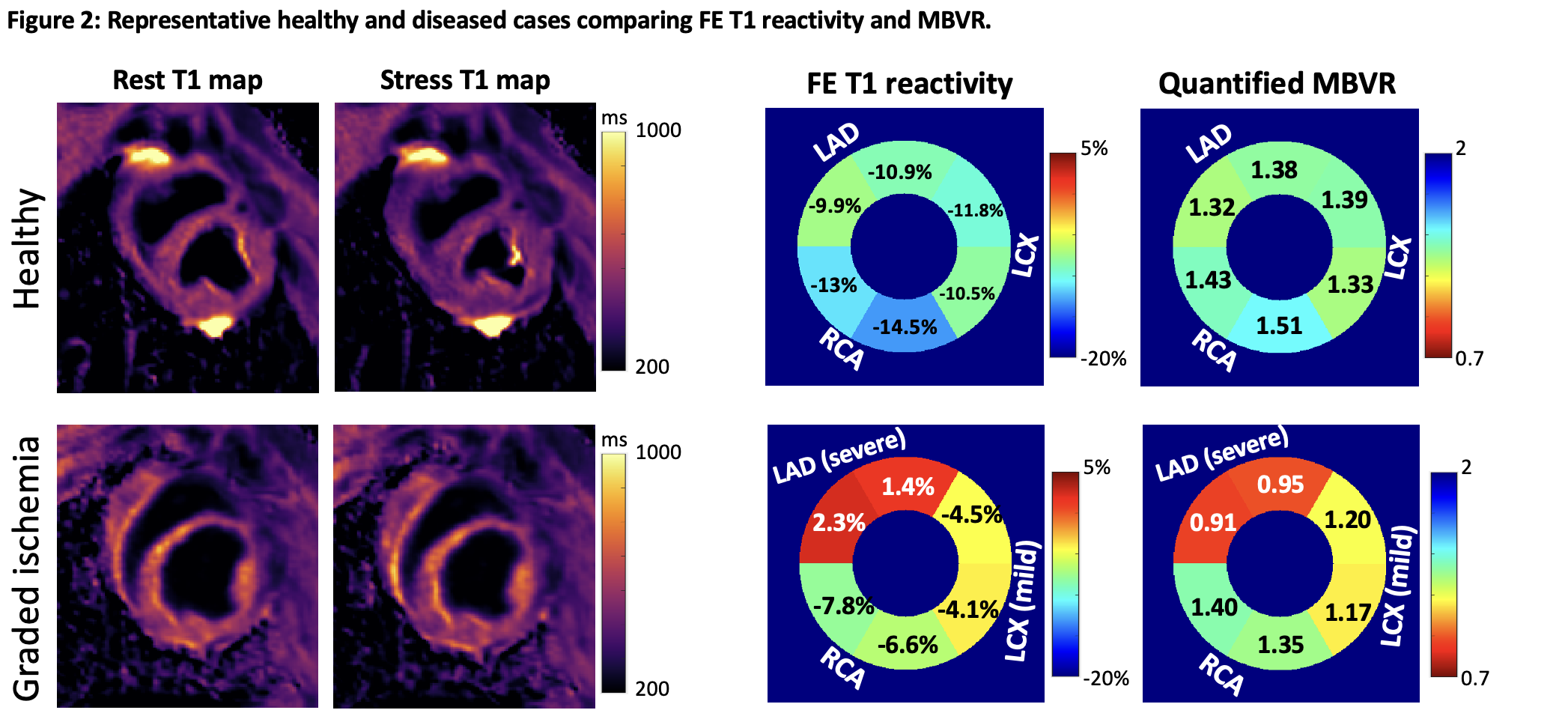 Figure 3. Comparison of in vivo findings highlighting the effectiveness of ferumoxytol-enhanced (FE) T1 reactivity and the proposed MBV reserve (MBVR) in distinguishing between healthy and ischemic myocardial tissue. (A) In regions supplied by healthy coronary arteries (green dots), the average FE T1 reactivity was −8.5% ± 3.2%, whereas ischemic regions (red dots) showed a reduced response of −2.5% ± 3.7%, with a statistically significant difference (p < 10⁻⁴). Likewise, MBVR values were notably higher in healthy areas (1.40 ± 0.10) compared to ischemic ones (1.08 ± 0.15), also with strong statistical significance (p < 10⁻⁴). (B) Receiver operating characteristic (ROC) analysis reveals that MBVR achieves a superior area under the curve (AUC = 0.97) for identifying myocardial ischemia, outperforming FE T1 reactivity (AUC = 0.89), with the difference reaching statistical significance (p < 0.05).
Figure 3. Comparison of in vivo findings highlighting the effectiveness of ferumoxytol-enhanced (FE) T1 reactivity and the proposed MBV reserve (MBVR) in distinguishing between healthy and ischemic myocardial tissue. (A) In regions supplied by healthy coronary arteries (green dots), the average FE T1 reactivity was −8.5% ± 3.2%, whereas ischemic regions (red dots) showed a reduced response of −2.5% ± 3.7%, with a statistically significant difference (p < 10⁻⁴). Likewise, MBVR values were notably higher in healthy areas (1.40 ± 0.10) compared to ischemic ones (1.08 ± 0.15), also with strong statistical significance (p < 10⁻⁴). (B) Receiver operating characteristic (ROC) analysis reveals that MBVR achieves a superior area under the curve (AUC = 0.97) for identifying myocardial ischemia, outperforming FE T1 reactivity (AUC = 0.89), with the difference reaching statistical significance (p < 0.05).