Congenital Track
Virtual Recording

Thomas M. Vollbrecht, MD
Physician
University Hospital Bonn
Bonn, Nordrhein-Westfalen, Germany
Thomas M. Vollbrecht, MD
Physician
University Hospital Bonn
Bonn, Nordrhein-Westfalen, Germany
Christopher Hart, MD
Pediatric Cardiologist
University Hospital Bonn, Germany

Alexander Isaak, MD
Managing Senior Physician
University Hospital Bonn
Bonn, Nordrhein-Westfalen, Germany
Annegret Geipel, MD
Prenatal Medicine Specialist
University Hospital Bonn
Bonn, Nordrhein-Westfalen, Germany

Julian A. Luetkens, MD
Physician
University Hospital Bonn
Bonn, Nordrhein-Westfalen, Germany
 Fetal 4D flow pathline visualizations with time-velocity curves in a fetus without congenital heart disease (CHD) and in fetuses with the two most common cyanotic heart defects: tetralogy of Fallot (TOF) and d-transposition of the great arteries (d-TGA). In the fetus without CHD, most descending aorta (Dao) flow passes through the main pulmonary artery (MPA) and ductus arteriosus (DA), with a smaller portion via the ascending aorta (AAo) and distal aortic arch (AA). Conversely, in TOF, pulmonary obstruction directs most combined ventricular output (CVO) through the AA, while in d-TGA, discordant ventricular-arterial connections cause a similar pattern. A key advantage of 4D flow over other flow imaging techniques is its ability to simultaneously depict anatomical features throughout the entire circulation: in the fetus without CHD, the AA and DA are nearly equal in size, whereas in TOF, reduced pulmonary blood flow is reflected in the smaller DA compared to the AA. Normal crossing pattern of the AAo and MPA is evident in the fetus without CHD and in TOF, while in d-TGA, the great arteries are parallel, obscuring the inferior DA and left pulmonary artery (LPA) from cranial views, while the right pulmonary artery (RPA) to the right remains visible.
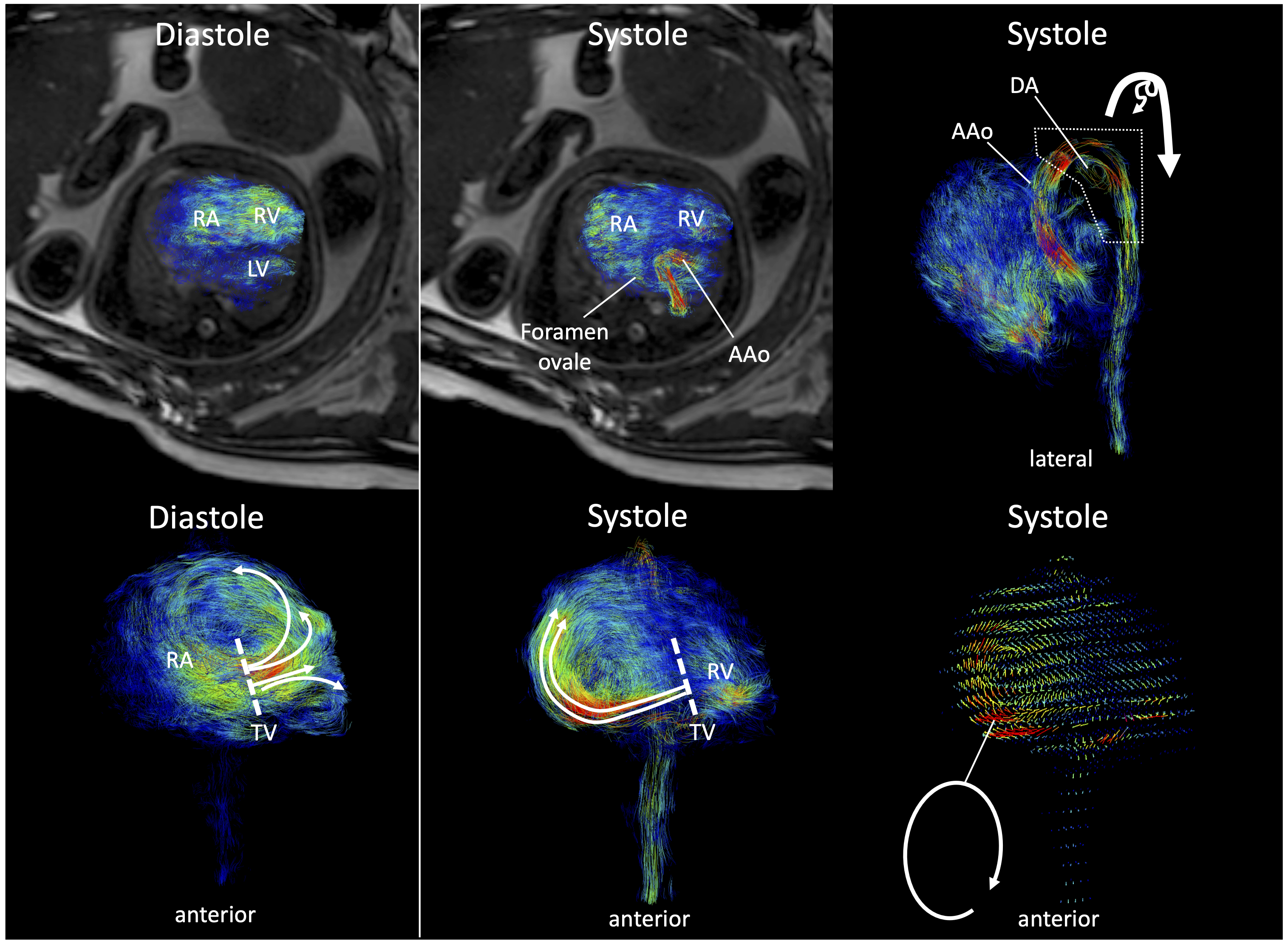
Fetal 4D flow pathline visualizations with time-velocity curves in a fetus without congenital heart disease (CHD) and in fetuses with the two most common cyanotic heart defects: tetralogy of Fallot (TOF) and d-transposition of the great arteries (d-TGA). In the fetus without CHD, most descending aorta (Dao) flow passes through the main pulmonary artery (MPA) and ductus arteriosus (DA), with a smaller portion via the ascending aorta (AAo) and distal aortic arch (AA). Conversely, in TOF, pulmonary obstruction directs most combined ventricular output (CVO) through the AA, while in d-TGA, discordant ventricular-arterial connections cause a similar pattern. A key advantage of 4D flow over other flow imaging techniques is its ability to simultaneously depict anatomical features throughout the entire circulation: in the fetus without CHD, the AA and DA are nearly equal in size, whereas in TOF, reduced pulmonary blood flow is reflected in the smaller DA compared to the AA. Normal crossing pattern of the AAo and MPA is evident in the fetus without CHD and in TOF, while in d-TGA, the great arteries are parallel, obscuring the inferior DA and left pulmonary artery (LPA) from cranial views, while the right pulmonary artery (RPA) to the right remains visible.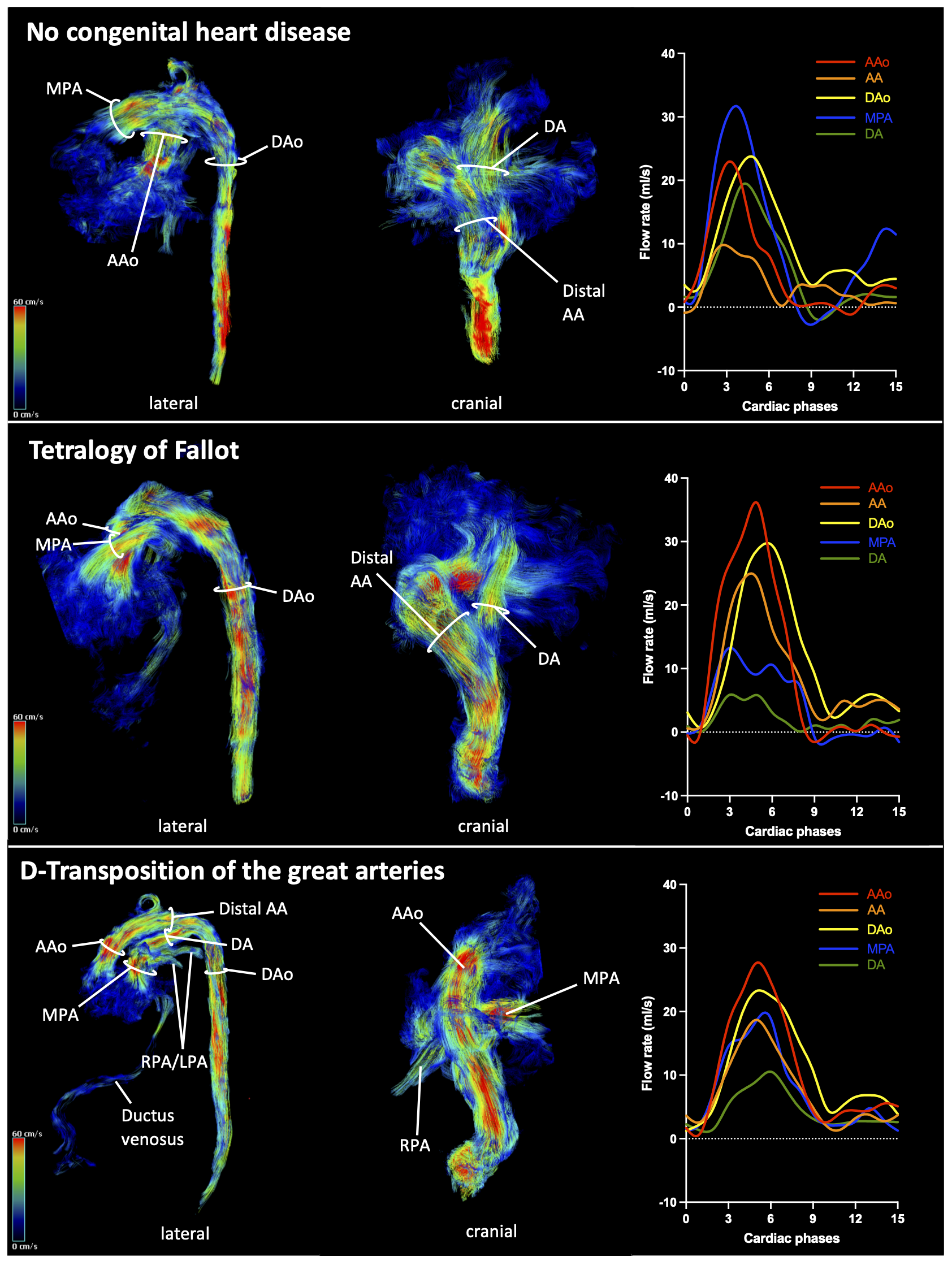 Images from a fetus with severe Ebstein anomaly and a circular shunt at 36 weeks of gestation (fetus 31). Diastole: (Top) 4D flow pathline visualization and axial cine overlay shows filling of the left ventricle (LV) and the enlarged right ventricle (RV). (Bottom) An anterior 4D flow pathline view highlights blood flow distribution from the right atrium (RA) across the anteriorly displaced tricuspid valve (TV), primarily directed cranially toward the right ventricular outflow tract. Systole: (Top left) The LV ejects blood into the ascending aorta (AAo), while RV blood predominantly regurgitates back into the RA via the insufficient TV, crossing the foramen ovale into the left heart. (Top right) Pathline visualization reveals absent antegrade flow in the main pulmonary artery and retrograde perfusion of the hypoplastic ductus arteriosus (DA) from the aortic arch, forming a circular shunt pathway (AAo → DA → RA → foramen ovale → LV → AAo). (Bottom left) Pathline visualization and (bottom right) velocity vectors depict massive retrograde flow from the RV into the RA through the insufficient TV, generating a prominent vortical flow pattern within the RA. The ability to visualize complex, multidirectional flow patterns enabled the identification of the circular shunt in this fetus, which would likely have been missed using 2D flow imaging alone.
Images from a fetus with severe Ebstein anomaly and a circular shunt at 36 weeks of gestation (fetus 31). Diastole: (Top) 4D flow pathline visualization and axial cine overlay shows filling of the left ventricle (LV) and the enlarged right ventricle (RV). (Bottom) An anterior 4D flow pathline view highlights blood flow distribution from the right atrium (RA) across the anteriorly displaced tricuspid valve (TV), primarily directed cranially toward the right ventricular outflow tract. Systole: (Top left) The LV ejects blood into the ascending aorta (AAo), while RV blood predominantly regurgitates back into the RA via the insufficient TV, crossing the foramen ovale into the left heart. (Top right) Pathline visualization reveals absent antegrade flow in the main pulmonary artery and retrograde perfusion of the hypoplastic ductus arteriosus (DA) from the aortic arch, forming a circular shunt pathway (AAo → DA → RA → foramen ovale → LV → AAo). (Bottom left) Pathline visualization and (bottom right) velocity vectors depict massive retrograde flow from the RV into the RA through the insufficient TV, generating a prominent vortical flow pattern within the RA. The ability to visualize complex, multidirectional flow patterns enabled the identification of the circular shunt in this fetus, which would likely have been missed using 2D flow imaging alone.