Quick Fire Session
Giuseppe Rovere, MD
Medical Doctor, Diagnostic Radiologist
Fondazione Policlinico Universitario "A.Gemelli" - IRCCS, Rome (Italy)
Rome, Lazio, Italy
Giuseppe Rovere, MD
Medical Doctor, Diagnostic Radiologist
Fondazione Policlinico Universitario "A.Gemelli" - IRCCS, Rome (Italy)
Rome, Lazio, Italy
Alessandro Marchetti, MD
Medical Doctor, Radiology Resident
Catholic University of Rome “Agostino Gemelli" University Polyclinic Foundation IRCCS
Roma, Lazio, Italy
Pietro Sciaccotta
Medical Doctor, Radiology resident
Catholic University of Rome “Agostino Gemelli" University Polyclinic Foundation IRCCS, Italy
Martina Schiavo
Medical Doctor, resident radiologist
Catholic University of Rome “Agostino Gemelli" University Polyclinic Foundation IRCCS, Italy

Francesco Lauriero, MD
Medical Doctor, Diagnostic Radiologist
Fondazione Policlinico Universitario "A. Gemelli" - IRCCS, Rome (Italy)
Rome, Lazio, Italy
Agostino Meduri, MD
Assistant Professor
Catholic University of Rome, "Agostino Gemelli" University Polyclinic Foundation IRCCS- Rome (Italy), Italy

Luigi Natale, MD
Medical Doctor, Associate Professor of Radiology
Catholic University - Fondazione Policlinico Universitario "A. Gemelli" IRCCS, Rome (Italy)
Rome, Lazio, Italy
Riccardo Marano, MD
Medical Doctor, Associate Professor of Radiology
Università Cattolica - Fondazione Policlinico Universitario "Agostino Gemelli" - IRCCS, Rome (Italy)
Rome, Lazio, Italy
Sequence | Plane / Coverage | Slice Thickness |
b-SSFP cine | 2-chamber, 4-chamber and short-axis views | 8 mm |
Axial T1W-BB | Transaxial, whole thorax | 5 mm |
Axial T1W-BB FS | Transaxial, whole thorax | 5 mm |
T2W-STIR | Best plane for mass study (usually short-axis view) | 5 mm |
Native T1 Mapping (MOLLI) | Short-axis view | 10mm (1-2 slices including the mass) |
T2 Mapping (mGraSE) | Short-axis view | 10mm (1-2 slices including the mass) |
First-pass perfusion (rest) | 3 short-axis slices + 1 2-chamber and 4 chamber slice | 10 mm |
EGE | Best plane for mass study (TI 500-550 ms; 2 min after contrast injection) | 5 mm |
FSPGR-3D T1W post-contrast | Whole heart | 2 mm |
LGE | 2-chamber, 4-chamber and short-axis views | 8 mm |
T1 Mapping enhanced (MOLLI) | Short-axis view | 10mm (1-2 slices including the mass) |
 (a) to (d) first pass rest perfusion images show no enhancement of the lesion in the RV (a) and LV (b) cavity phases. Just after the LV phase (c) a focal area of enhancement can be seen along the posterior wall, persisting into the myocardial phase (d); the same area can be seen in FSPGR T1W post-contrast (e) and delayed enhancement (f) images. Ischemic LGE along the basal lateral wall of the left ventricle, extending into the medium infero-lateral wall is also observed.
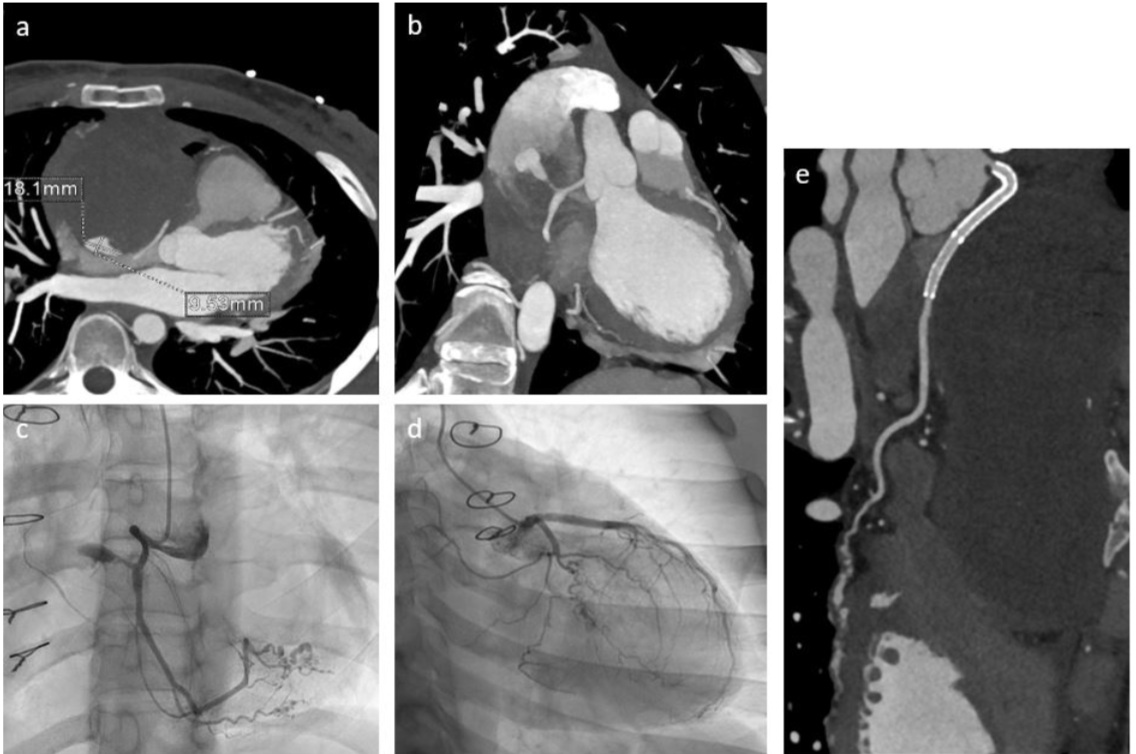
(a) to (d) first pass rest perfusion images show no enhancement of the lesion in the RV (a) and LV (b) cavity phases. Just after the LV phase (c) a focal area of enhancement can be seen along the posterior wall, persisting into the myocardial phase (d); the same area can be seen in FSPGR T1W post-contrast (e) and delayed enhancement (f) images. Ischemic LGE along the basal lateral wall of the left ventricle, extending into the medium infero-lateral wall is also observed.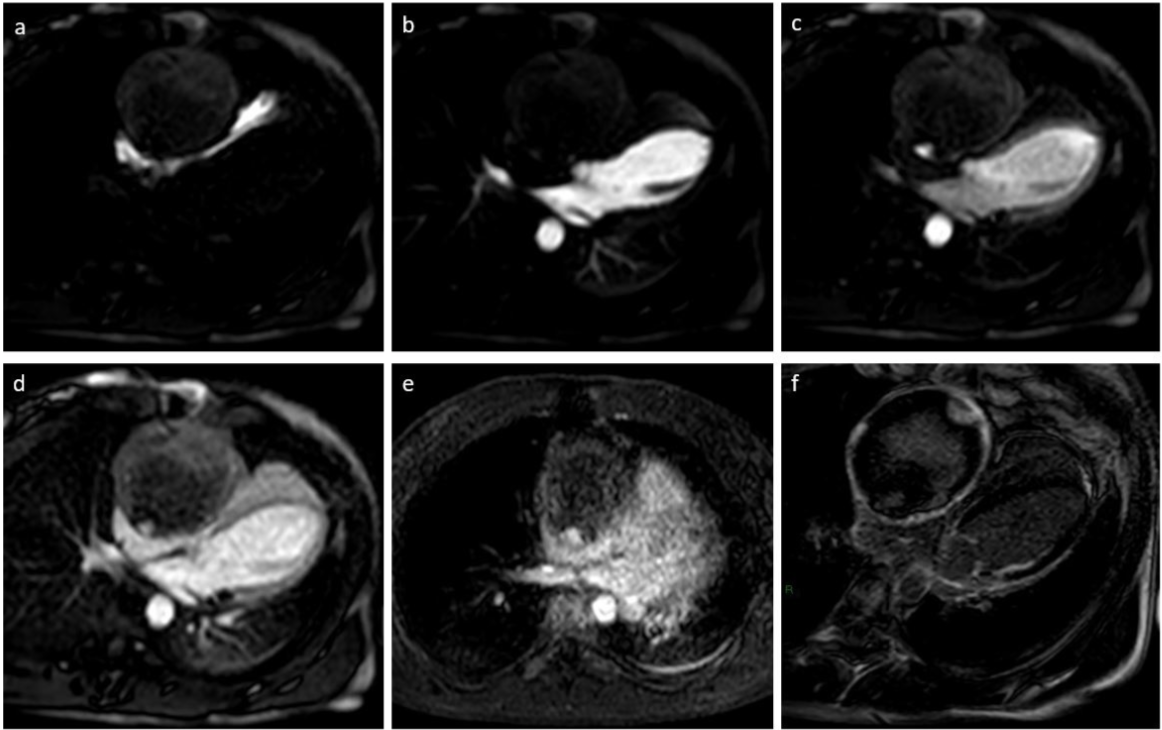 Axial (a) and coronal (b) MIP reformat images from CCT show a focal area of enhancement within the peripheric portion of the lesion, communicating with the right coronary artery trough a slender acute marginal branch/atrial branch; the same finding is confirmed by invasive coronary angiography (c-d) which also shows multiple stenosis with ectasia of intervening tracts of the right postero-lateral branch, the distal portion of posterior descending artery, and an obtuse marginal branch of LCX. Follow-up CTA after PCI shows patency of the overlapping stents in the proximal tract of RCA, with complete exclusion of the pseudoaneurysm.
Axial (a) and coronal (b) MIP reformat images from CCT show a focal area of enhancement within the peripheric portion of the lesion, communicating with the right coronary artery trough a slender acute marginal branch/atrial branch; the same finding is confirmed by invasive coronary angiography (c-d) which also shows multiple stenosis with ectasia of intervening tracts of the right postero-lateral branch, the distal portion of posterior descending artery, and an obtuse marginal branch of LCX. Follow-up CTA after PCI shows patency of the overlapping stents in the proximal tract of RCA, with complete exclusion of the pseudoaneurysm.